Every year, more than 20,000 children experience cardiac arrest in the United States. Yet many people assume performing BLS in kids simply means scaling down adult techniques. This dangerous misconception can cost precious lives.
Children aren’t miniature adults. Their physiology, cardiac arrest causes, and resuscitation needs differ dramatically. Understanding these differences can mean the difference between life and death.
What Is Considered a Kid in BLS?
When it comes to BLS in kids, age definitions matter significantly. According to the 2025 American Heart Association guidelines, pediatric patients are categorized into specific groups.
Infants include children younger than approximately 1 year of age. Children are defined as approximately 1 year of age until puberty. For teaching purposes, puberty is identified by breast development in females and axillary hair presence in males.
Anyone showing signs of puberty follows adult BLS protocols. This age-based approach ensures rescuers apply appropriate techniques for each developmental stage.
The distinction exists because body size, chest wall compliance, and underlying arrest causes vary significantly across these age groups. Newborns require separate neonatal resuscitation protocols and aren’t included in pediatric BLS guidelines.
Understanding Pediatric BLS Fundamentals
Basic life support in kids focuses on different priorities than adult resuscitation. Most pediatric cardiac arrests stem from respiratory causes rather than primary cardiac events.
Asphyxia, respiratory failure, and progressive shock commonly trigger pediatric arrests. This fundamental difference shapes every aspect of pediatric BLS protocols.
Research shows that compression-ventilation CPR with ratios of 15:2 or 30:2 demonstrates better outcomes compared with compression-only CPR in children. Effective ventilation becomes paramount during pediatric resuscitation.
The 2025 guidelines emphasize high-quality CPR components. These include adequate compression rate and depth, minimizing interruptions, allowing complete chest recoil, and avoiding excessive ventilation.
For children, compressions should reach at least 2 inches deep or one-third of the chest diameter. Infants require approximately 1.5 inches of depth. Both groups need 100-120 compressions per minute.
Why Is the CPR Ratio Different for Kids?
The CPR ratio differs for kids because their cardiac arrest etiology fundamentally differs from that of adults. Children primarily experience respiratory arrest that progresses to cardiac arrest.
Adult cardiac arrests typically result from sudden cardiac events like ventricular fibrillation. Children rarely experience these rhythms. Pediatric out-of-hospital cardiac arrest survival remains around 10%, with complex resuscitation needs possibly contributing to the lack of improvement.
Single rescuer pediatric BLS uses a 30:2 compression-to-ventilation ratio. This matches adult CPR for educational simplicity and easier skill retention across age groups.
Two or more rescuers should use a 15:2 ratio for BLS in kids. This increased ventilation frequency addresses the respiratory nature of pediatric arrests while maintaining adequate perfusion.
The two-finger technique for infant compressions is no longer recommended. Rescuers should use the heel of one hand or the two-thumb encircling hands technique instead.
Healthcare providers must minimize compression interruptions to less than 10 seconds. Every pause reduces crucial blood flow to vital organs, particularly the developing brain.
Advanced Techniques for BLS in Kids
Proper hand positioning varies by patient size during BLS in kids. Small children may only require one hand for chest compressions. Larger children might need two hands, similar to adult techniques.
Rescuers must position themselves appropriately. Being too low reduces compression effectiveness. Standing on stools or raising the bed height optimizes mechanical advantage.
The compression-airway-breathing sequence mirrors adult protocols for training consistency. However, if the arrest was witnessed and deemed cardiac in origin, calling for help before starting compressions takes priority.
The 2025 guidelines represent the first comprehensive update of treatment recommendations since 2020. These updates incorporate extensive evidence reviews from international resuscitation committees.
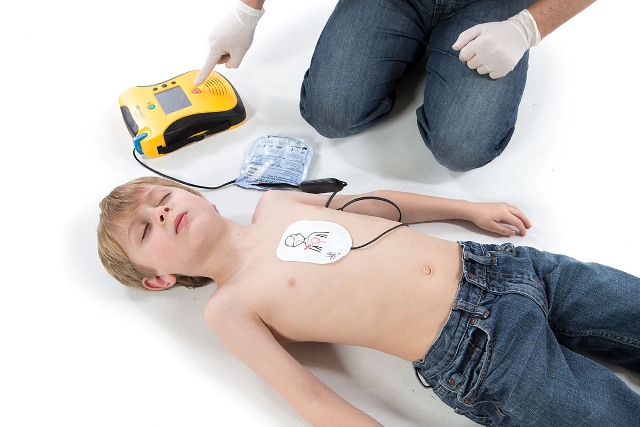
Automated external defibrillators should be applied immediately when available. Pediatric pads or settings are preferred. However, adult pads may be used if pediatric options aren’t accessible.
Can You Perform CPR on Kids?
Absolutely. Anyone can and should perform CPR on kids experiencing cardiac arrest. Early bystander CPR significantly improves survival outcomes.
Findings show that less than 40 percent of adults receive CPR from a layperson. This statistic is even more tragic for children, where every second counts.
If you’re alone with a child in cardiac arrest, start CPR immediately. After five cycles (approximately two minutes), you can briefly leave to call 911 if no one else is available.
For infants, check for responsiveness by tapping the foot. Avoid shaking, which could cause injury. If unresponsive with no normal breathing, begin CPR immediately.
Children aged 12 years and older can now be trained to perform CPR and use AEDs according to updated guidelines. Teaching young people these skills creates more potential rescuers.
Remember that doing something is always better than doing nothing. Even imperfect CPR provides some blood flow and oxygen to vital organs.
Survival Statistics and Outcomes
In-hospital pediatric cardiac arrest outcomes have improved significantly. Survival increased from 19% in 2000 to 38% in 2018 for pulseless cardiac arrests. However, survival rates plateaued after 2010.
Out-of-hospital survival remains challenging. Factors affecting outcomes include witnessed arrests, early bystander CPR, and return of spontaneous circulation before hospital arrival.
More than 19,000 pediatric in-hospital cardiac arrests occur per year in the United States. This represents 1-2% of all hospitalized children annually.
Survival varies by underlying conditions. Children with surgical cardiac issues show higher survival rates than those with medical cardiac conditions or non-cardiac causes.
Early recognition, immediate high-quality CPR, and rapid access to advanced care dramatically improve outcomes. Every minute without CPR decreases survival chances by approximately 10%.
Key Differences in Pediatric BLS Protocols
Several critical differences distinguish BLS in kids from adult protocols:
Respiratory Focus: Children need rescue breaths due to respiratory arrest causes. Compression-only CPR isn’t recommended for pediatric patients.
Compression Depth: Scaled to one-third of chest depth rather than fixed measurements, ensuring appropriate force for varying body sizes.
Rescue Breathing Rate: A respiratory rate of 20 to 30 breaths per minute is recommended for infants and children receiving CPR with an advanced airway.
Initial Assessment: Healthcare providers may take up to 10 seconds to check for pulse in children, unlike the rapid adult assessment.
Defibrillation Energy: Pediatric patients require 2 joules per kilogram for initial defibrillation attempts.
These modifications reflect physiological differences between children and adults. Applying adult protocols to children can result in inadequate resuscitation.
Common Pediatric Cardiac Arrest Causes
Understanding why children experience cardiac arrest helps rescuers anticipate and prevent these emergencies.
Respiratory causes dominate pediatric arrests. Asthma, bronchiolitis, choking, drowning, and respiratory infections can all progress to cardiac arrest if untreated.
Trauma accounts for significant pediatric arrests, particularly in emergency departments. Falls, motor vehicle accidents, and abuse-related injuries trigger many cases.
Sudden cardiac death occurs less frequently in children but affects young athletes. A study of young athletes identified 132 cases with an overall survival rate of 48%, with higher survival when certified athletic trainers and on-site AEDs were involved.
Congenital conditions, including heart defects and genetic disorders,s increase cardiac arrest risk in certain populations.
Infections like sepsis can cause progressive shock leading to cardiac arrest in previously healthy children.
Prevention remains the best strategy. Recognizing early warning signs like respiratory distress, altered consciousness, or poor perfusion enables intervention before arrest occurs.
Take Action: Get Certified in Memphis
Understanding BLS in kids isn’t enough. Proper training builds confidence and competence for real emergencies. Lives depend on skilled rescuers who can act quickly and correctly.
CPR Memphis offers comprehensive American Heart Association training that prepares you for pediatric emergencies. Our stress-free, hands-on classes ensure you master techniques specific to infants and children.
Don’t wait for an emergency to wish you’d gotten CPR certification in Memphis. Our expert instructors guide you through realistic scenarios, building muscle memory that lasts.
We offer initial certifications and renewals in BLS for Healthcare Providers, ACLS, PALS, and CPR and First Aid courses. Every class emphasizes pediatric differences and proper technique application.
Whether you’re a healthcare provider needing BLS certification in Memphis or a parent wanting to protect your children, we have a course for you. Our American Heart Association training site maintains the highest standards.
Visit CPR Memphis today and join thousands who’ve gained life-saving skills. When a child’s life hangs in the balance, your training makes all the difference. Register now at our Memphis location and become the rescuer every child deserves.
Frequently Asked Questions About BLS in Kids
Q: At what age do children transition to adult CPR protocols?
Children showing signs of puberty follow adult BLS guidelines. For teaching purposes, this means breast development in females and axillary hair in males. The transition typically occurs between the ages of 10 and 14, but varies individually. When uncertain, using pediatric protocols is safer than adult techniques for smaller children.
Q: Why can’t we use compression-only CPR for children as we do for adults?
Pediatric cardiac arrests primarily result from respiratory causes, not sudden cardiac events. Children need rescue breaths to address the underlying oxygen deprivation that triggered their arrest. Compression-only CPR may work for adults with sudden cardiac collapse, but children require both compressions and ventilations for optimal outcomes. Studies consistently show better survival with compression-ventilation CPR in pediatric patients.
Q: How long should you perform CPR on a child before stopping?
Continue CPR until professional help arrives, the child shows signs of life, you become too exhausted to continue, or the scene becomes unsafe. Unlike adults, pediatric resuscitation often continues for a longer period because children have a greater recovery potential. Healthcare providers may continue CPR for extended periods, especially in certain circumstances like hypothermia or in-hospital arrests where advanced interventions are available. Never stop CPR prematurely without clear medical direction.